Inguinal Hernia
A hernia is one of the most common surgical conditions we treat. An inguinal hernia looks like a lump in the groin, more commonly in a boy. See below for more detailed information.
See this on your mobile


The Condition
What is an inguinal hernia?
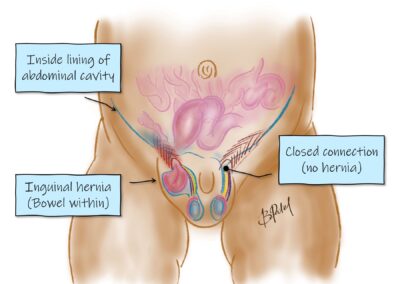
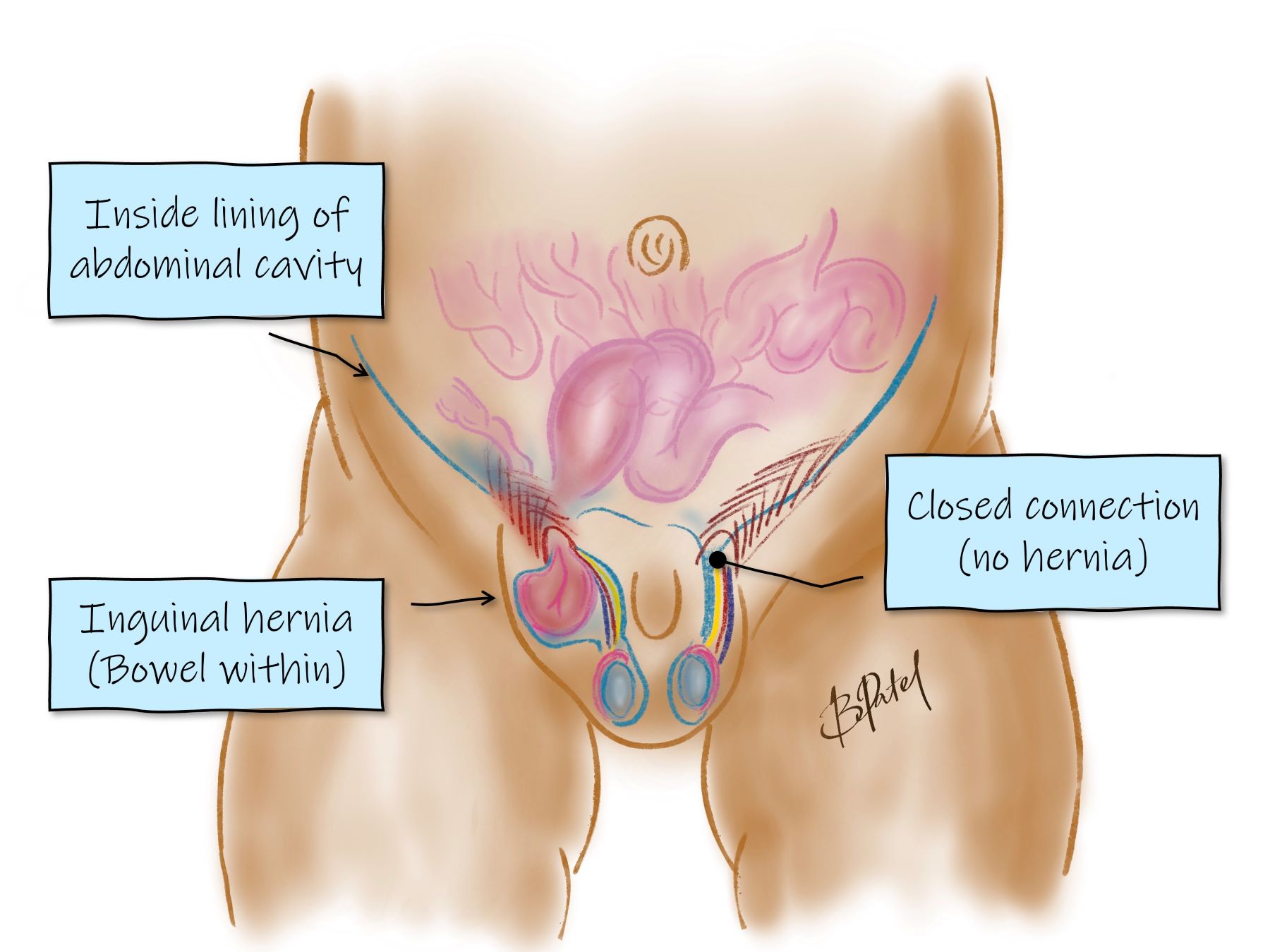
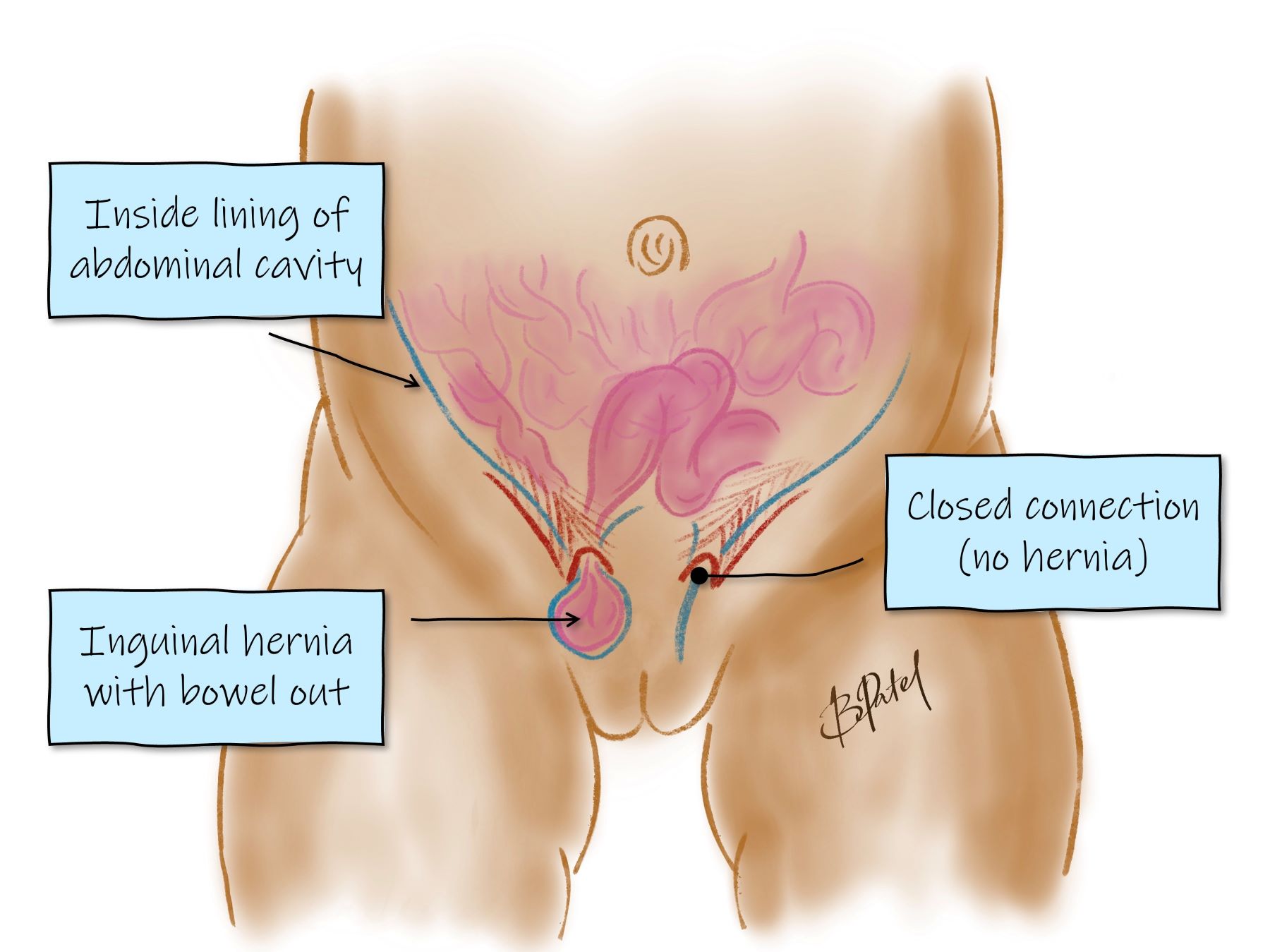
An inguinal hernia is a lump in the groin (inguinal region), often related to the intestines bulging through an opening in the abdominal muscles. It is more common in boys, as it relates to how the testicle descends into the scrotum. There is an opening into the groin,
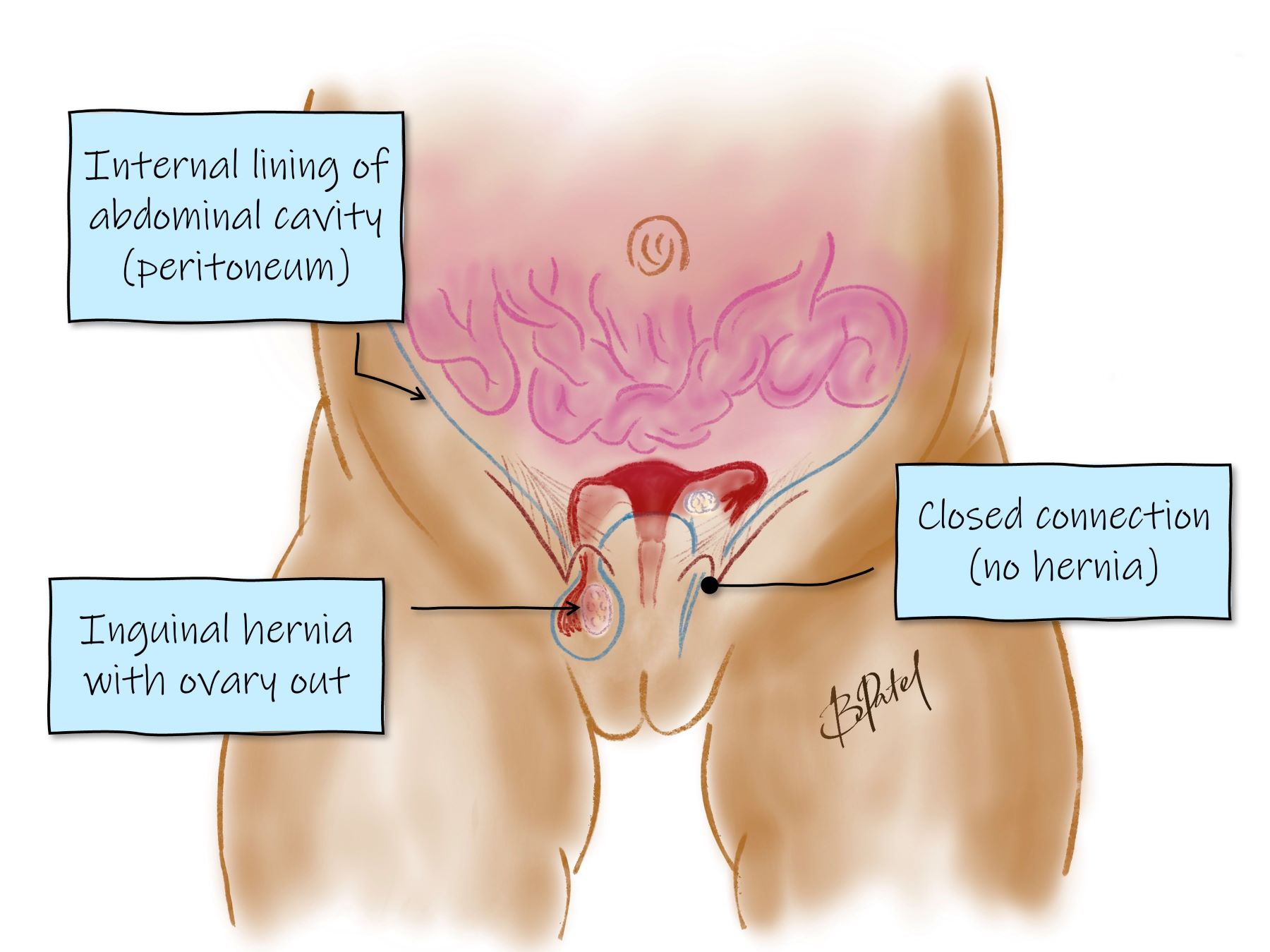
through which the intestine or internal fat can protrude. In girls the ovary and fallopian tube can protrude.
Children have different inguinal hernias to adults. There is no weakness that requires mesh.
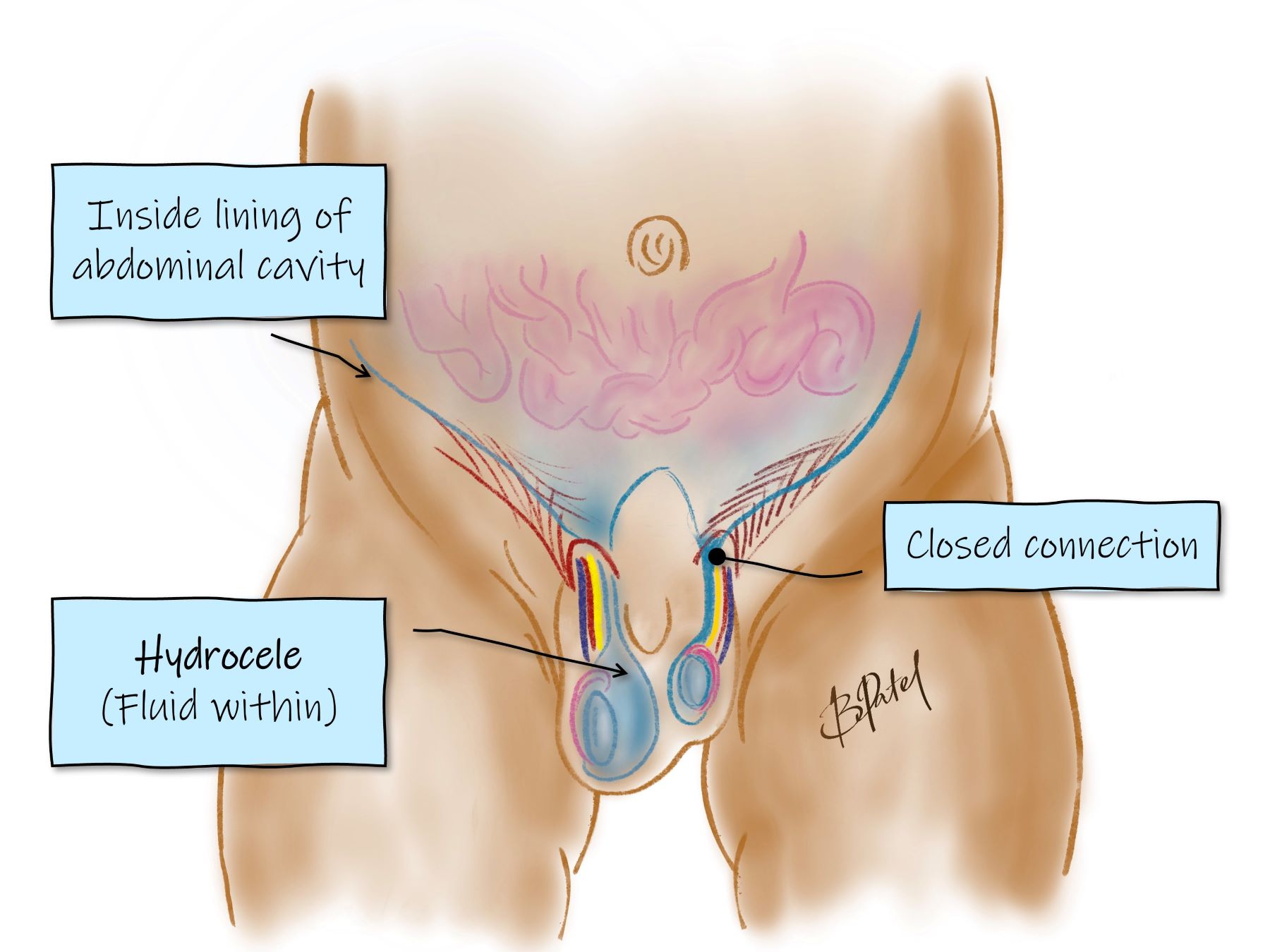
A hydrocele is a similar process, and only has fluid around the testis. It is usually visible all the time, whereas an inguinal hernia comes out with straining / crying.
-
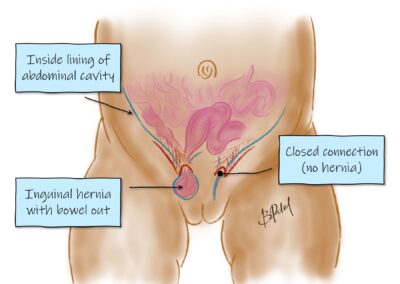
Inguinal hernia with bowel out
-
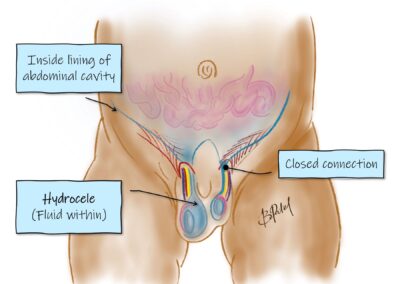
Hydrocele
-
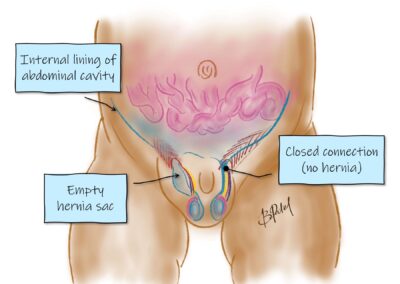
Inguinal hernia with empty sac
-
Inguinal hernia female
-
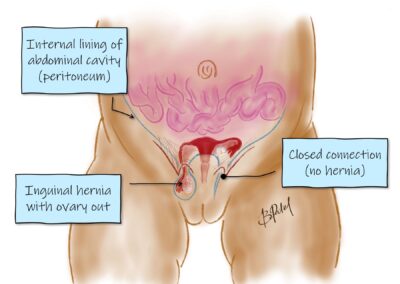
Inguinal hernia - ovary out
-
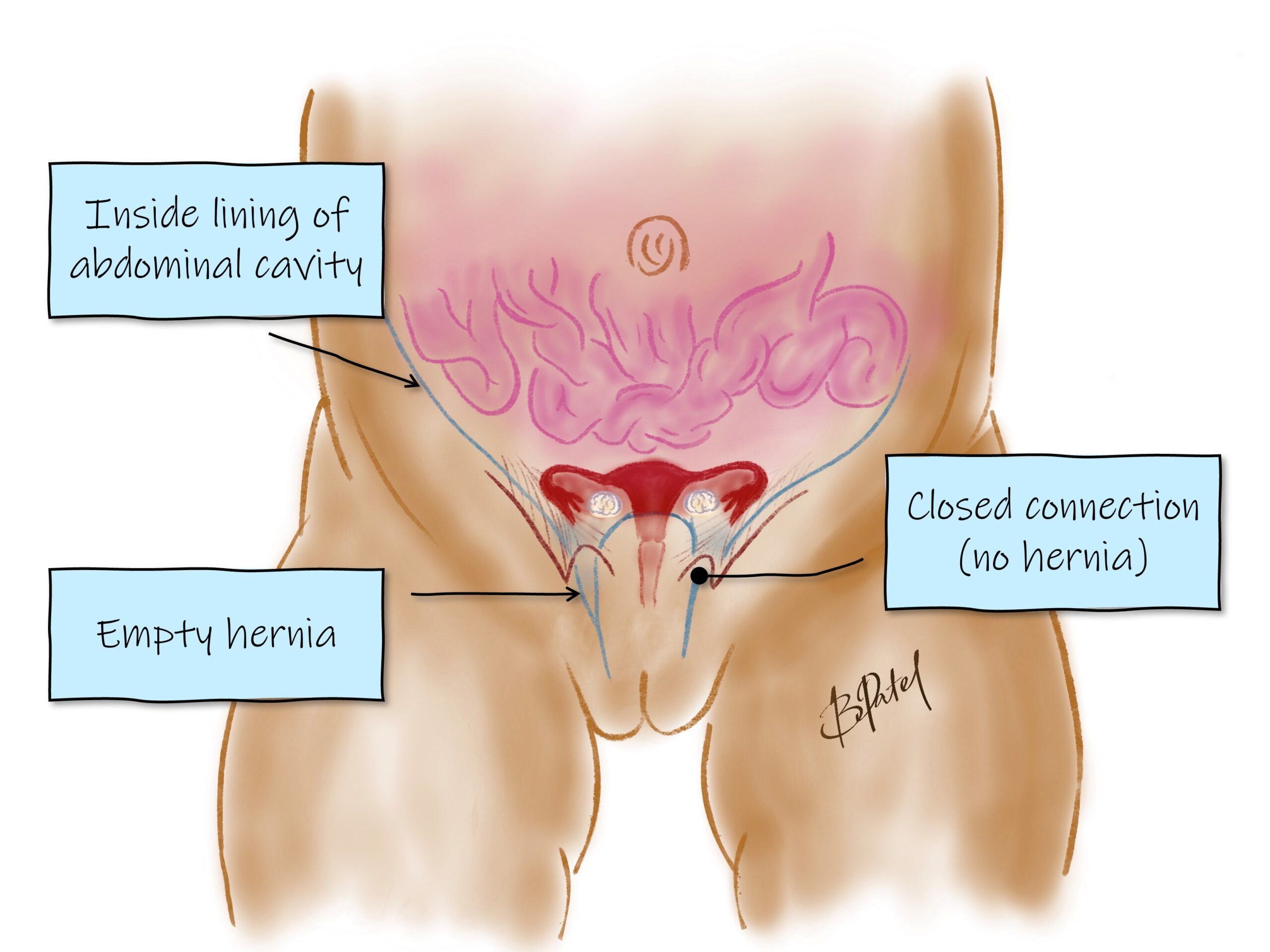
Inguinal hernia with empty sac - female
Why does it occur?
There is a delay or failure of closure of the track through which the testis (in boys) migrates to the scrotum during development. This opening allows abdominal contents such as bowel to bulge through the opening.
It is most often an isolated condition, although it can be associated with other medical conditions.
Premature infants have a higher risk of developing inguinal hernias due to immaturity of tissue development. Repair is often performed before discharge from the neonatal unit.
Does it need repair?
Yes. Inguinal hernias do not resolve on their own. Due to the risk to the intestine, testis or ovary it is worthwhile repairing once the diagnosis has been made. If the hernia becomes stuck or irreducible, an emergency repair may be required.
Is it dangerous?
It can be. Inguinal hernias cause trouble in about 10% of children.
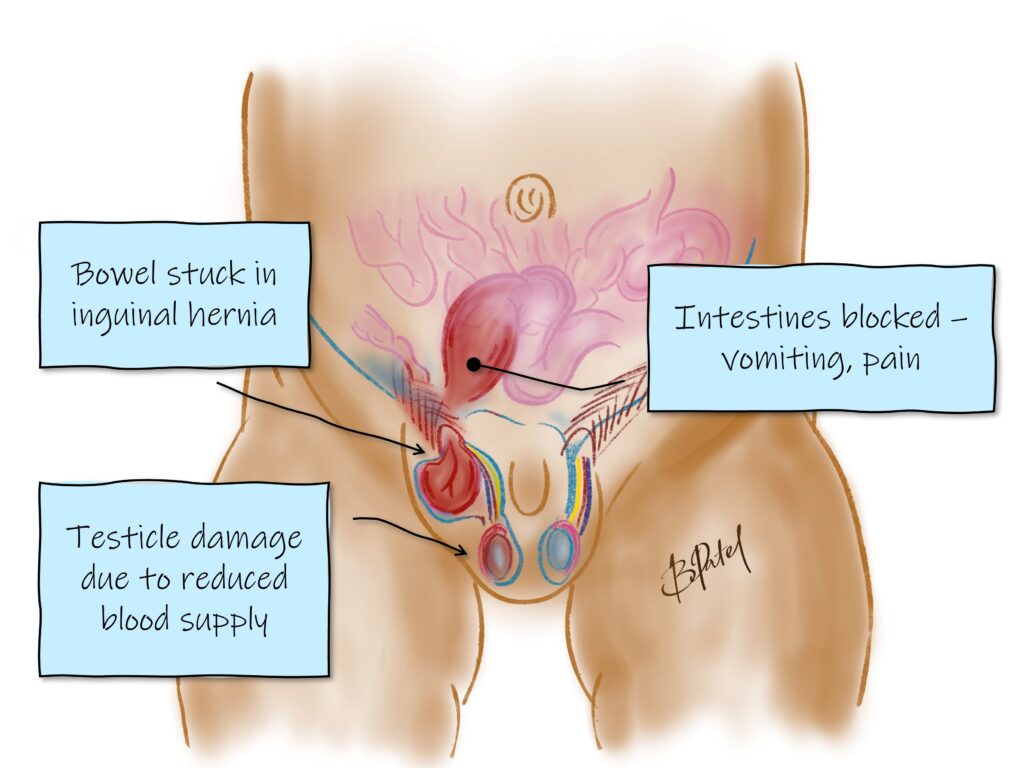
Irreducibility: There is a chance the hernia can become irreducible (also called incarcerated), and the contents become stuck and potentially injured (also called strangulated). It will look like a firm lump that doesn’t reduce, becomes tender and a little red. Vomiting may occur.
If this occurs please take your child to the nearest emergency centre for assessment. Do not give your child a feed. If it is an irreducible (or stuck) hernia, your child may need emergency surgery, which is much safer with an empty stomach.
A hydrocele is not dangerous. It often resolves after 1-2 years age. Persistent or new hydroceles may require surgery.
Treatment
Surgical repair
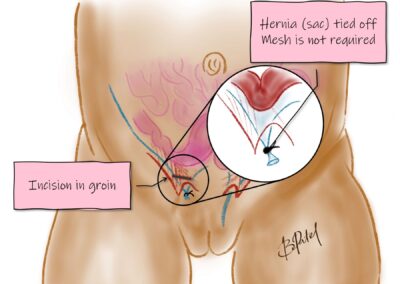
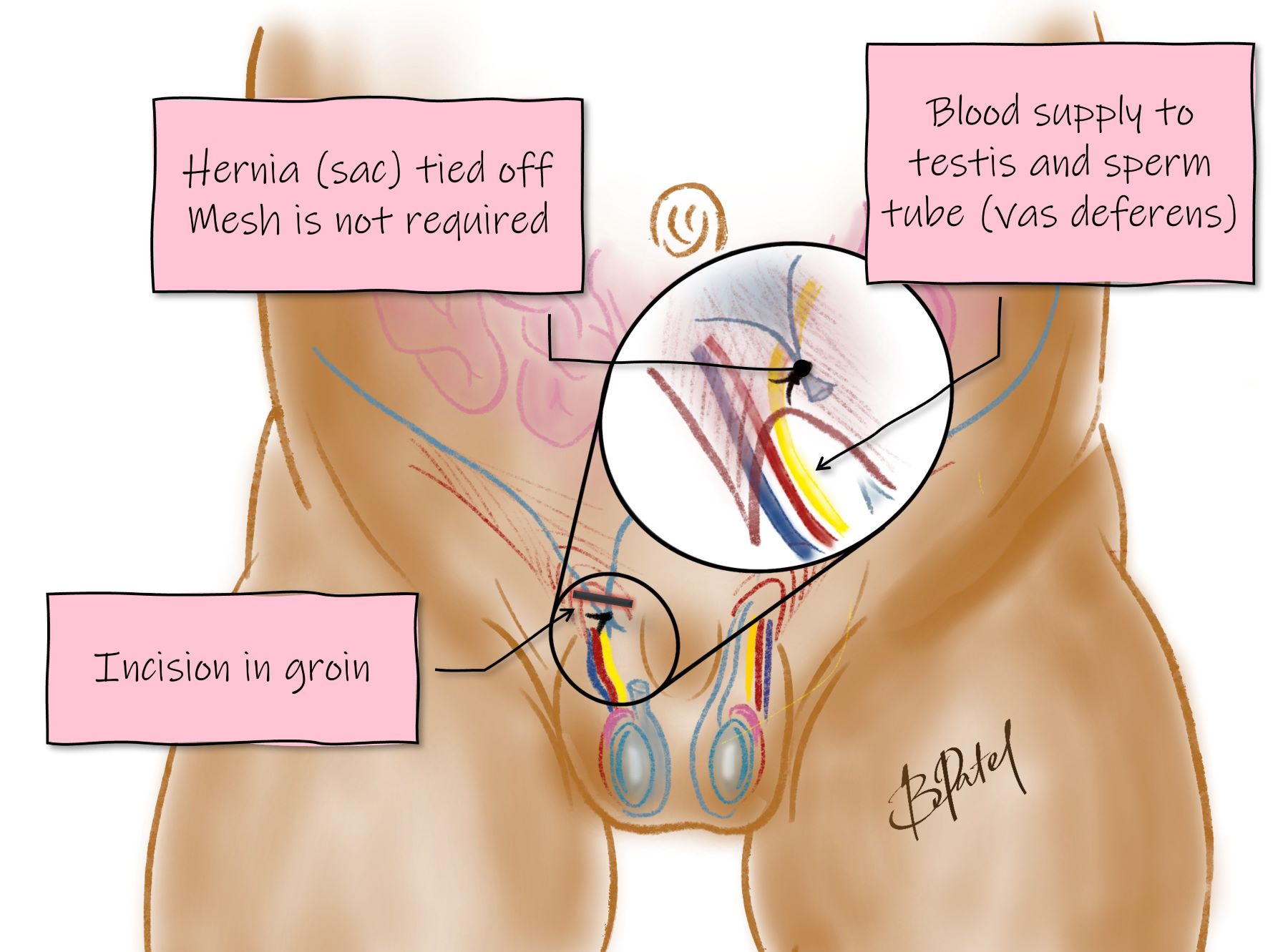
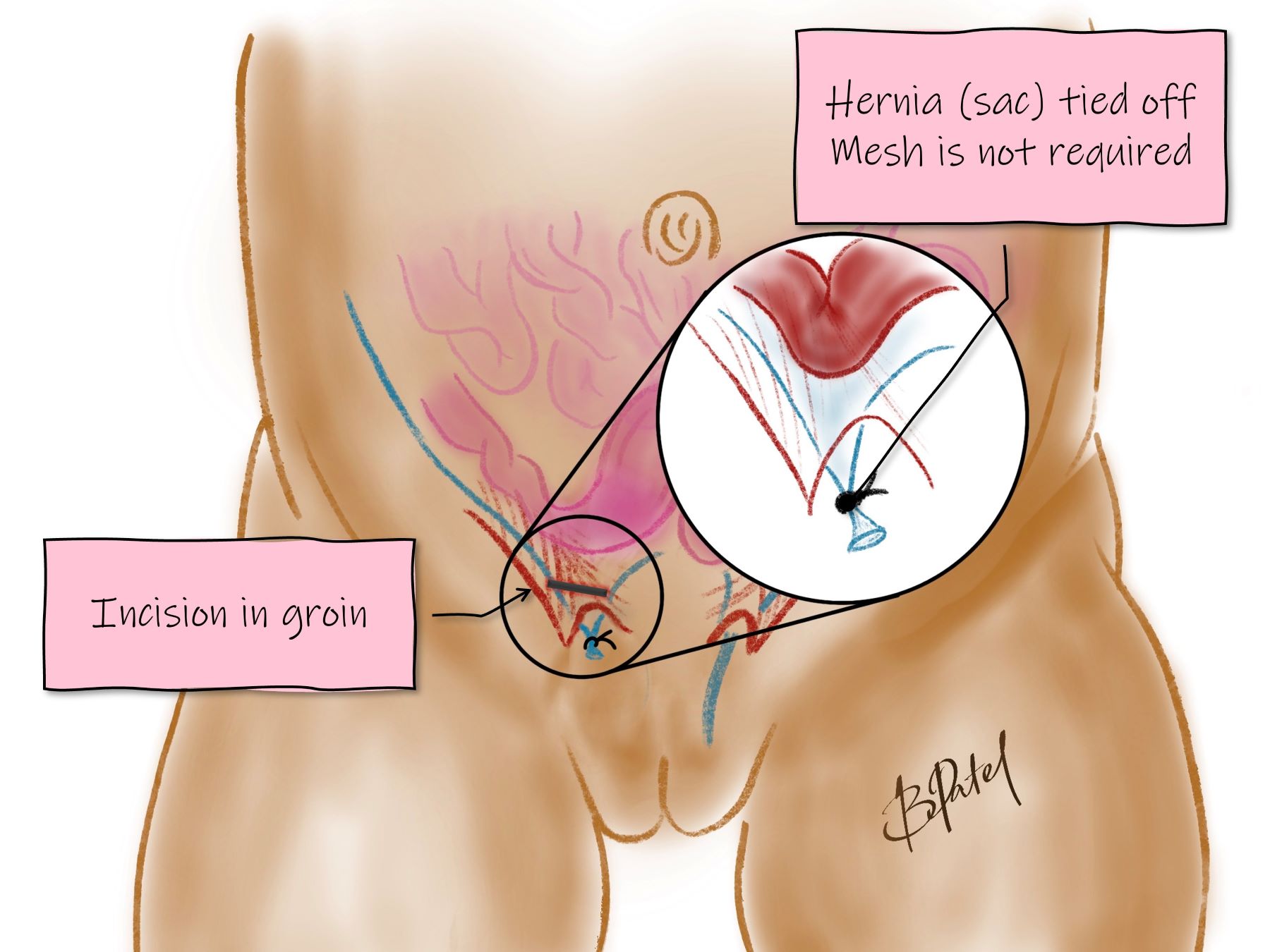
A day procedure under general anaesthetic, through a small incision in the groin. The hernia is closed with sutures, and the wound is closed with dissolvable sutures. There is no mesh.
-
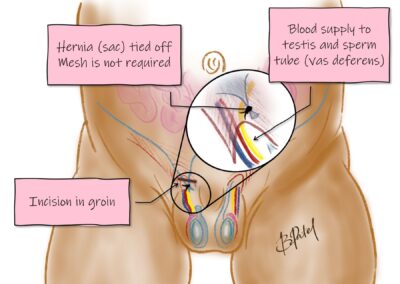
Inguinal hernia repair - male
-
Inguinal hernia repair - female
How long does the operation take?
The operation takes about 15-20 minutes.
The anaesthetic can take about the same time before and after, so you’ll be away from your child for an hour or so, until they are ready for you in the recovery room. You will be notified when they are ready for you to see them in recovery.
Should I repair the other side too?
Your surgeon will speak to you about options. There is a chance of developing a hernia on the other side, and depending on your child’s risk factors may be worthwhile exploring both sides.
What are the risks of the operation?
The anaesthetic – airway and breathing issues are extremely rare
- Recurrence – about 1% for most children, more often in premature infants.
- Injury to structures – the testicle, blood vessels and the vas deferens may be injured very rarely, especially in premature infants. Bowel injury is possible if the hernia is strangulated (stuck). In a girl the ovary or fallopian tube may be injured if it was protruding.
- Infection -1%
- Bleeding, bruising and swelling. Usually minor.
Recovery
What happens after the operation?
Recovery – you will be called into the recovery room just after they are awake.
Feeding – you can give your child a feed in the recovery room.
Home – usually after an hour or 2, once the nursing team have ensured your child is safe and comfortable
The wound / Dressings
The area will become swollen, and a little firm under the wound. This is a normal healing process and developing scar. The scar becomes dark red for the first few months, then becomes more pale.
There is a waterproof dressing in the groin that can be removed in the bath / shower after a week.
Expect some bruising / swelling after the operation. The dressing in the groin can be removed after 1 week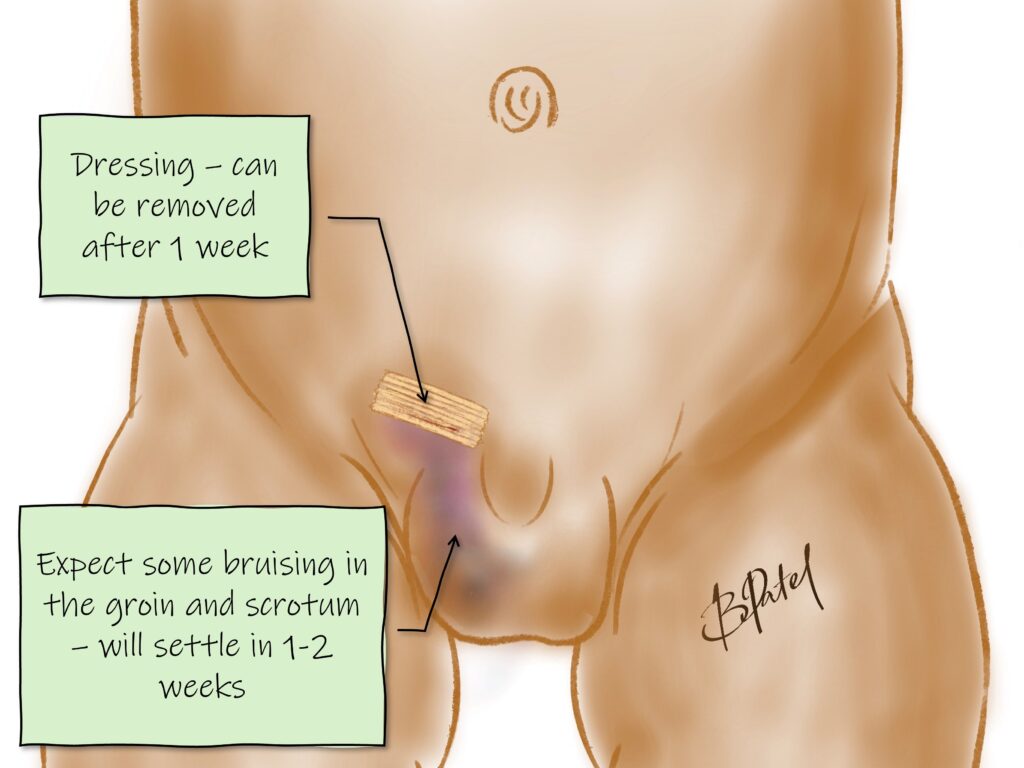
Pain relief
Your child will receive good pain relief in the operating room, that will last a few hours.
After the operation they will need paracetamol and possibly ibuprofen (eg. Nurofen) for a few days. Please let your surgeon and anaesthetist know if your child has intolerances or allergies.
In order to avoid medication, aim to distract your child and keep their mind off the area. Reading, writing, playing board games and other engaging activities help.
Normal activity
Bath / shower – the day after the operation
Swimming – 1 week
Daycare / School – 5-7 days
Sports – 2-3 weeks
Troubleshooting
The hernia is stuck
If you notice a bulge in the groin that is not reducing any more, it may be irreducible. If it stays this way for a few hours the content (bowel / testis / ovary) may become injured. This is called strangulation, and your child will require emergency treatment.
Try to stay calm, and take your child to the nearest children’s hospital. Do not give your child a feed, as it is safer for them to have an empty stomach. The emergency team and surgical team will look after your child.
Is there a wound infection?
Infections can develop around 2-4 days after the operation, and is a fairly uncommon issue.
The wound may be infected if there is increasing redness around the wound and tenderness. This may be associated with discharge from the wound site.
You will need to see your family doctor or call your surgeon for further advice.
It is very swollen - has it recurred?
It does become swollen after the operation, usually for a few days.
If your child has increasing pain, tenderness and vomiting associated with a similar bulge to before the operation there may be recurrence. If your child is unwell, you may need to go to the emergency department. Call your surgeon and let them know.
Otherwise see your GP and call your surgeon so your child can be assessed.
What do I look for?
You know your child best. If you have any concerns please see your family doctor or call your surgeon. The list below are issues that require medical attention.
- Increasing pain or persisting pain despite pain relief
- Increasing swelling or bulge – possible recurrence
- Fever >38.2 degrees Celsius
- Vomiting and feed intolerance
- Discharge or bleeding from the wound
- No bowel motions after 3 days
Experienced Surgeons
Over 25 years experience in paediatric surgery
Locations
Queensland and northern New South Wales
Appointments
Prioritised time for your child
Information
Conditions, procedures and aftercare
In the spirit of reconciliation we acknowledge the Traditional Custodians of country throughout Australia and their connections to land, sea and community. We pay our respect to their Elders past and present and extend that respect to all Aboriginal and Torres Strait Islander peoples.